false 0001671858 0001671858 2024-03-07 2024-03-07
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
March 7, 2024
Date of Report (Date of earliest event reported)
ARS Pharmaceuticals, Inc.
(Exact name of registrant as specified in its charter)
|
|
|
|
|
| Delaware |
|
001-39756 |
|
81-1489190 |
| (State or other jurisdiction of incorporation) |
|
(Commission File Number) |
|
(IRS Employer Identification No.) |
|
|
|
|
|
| 11682 El Camino Real, Suite 120 San Diego, California |
|
92130 |
| (Address of principal executive offices) |
|
(Zip Code) |
Registrant’s telephone number, including area code: (858) 771-9307
Not Applicable
(Former name or former address, if changed since last report.)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligations of the registrant under any of the following provisions:
| ☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
|
|
|
|
|
| Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
| Common Stock, $0.0001 par value per share |
|
SPRY |
|
The Nasdaq Stock Market LLC |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§ 230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§ 240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 2.02 |
Results of Operations and Financial Condition. |
On March 7, 2024, ARS Pharmaceuticals, Inc. (the “Company”) announced in its corporate presentation that as of December 31, 2023, it had approximately $228 million in cash and short-term investments.
The information in this Item 2.02 of this Current Report on 8-K is furnished and shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act of 1933, as amended (the “Securities Act”). The information shall not be deemed incorporated by reference into any other filing with the Securities and Exchange Commission made by the Company, whether made before or after today’s date, regardless of any general incorporation language in such filing, except as shall be expressly set forth by specific references in such filing.
| Item 7.01. |
Regulation FD Disclosure. |
On March 7, 2024, the Company updated its corporate presentation for use in meetings with investors, analysts and others. The presentation is available through the Company’s website and a copy is attached as Exhibit 99.1 to this Current Report on Form 8-K and incorporated by reference herein.
The information in this Item 7.01 of this Current Report on 8-K, including Exhibit 99.1, is furnished and shall not be deemed “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act. The information shall not be deemed incorporated by reference into any other filing with the Securities and Exchange Commission made by the Company, whether made before or after today’s date, regardless of any general incorporation language in such filing, except as shall be expressly set forth by specific references in such filing.
| Item 9.01 |
Financial Statements and Exhibits. |
(d) Exhibits
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
|
|
|
|
|
|
| Date: March 7, 2024 |
|
|
|
ARS Pharmaceuticals, Inc. |
|
|
|
|
|
|
|
|
By: |
|
/s/ Richard Lowenthal, M.S., MBA |
|
|
|
|
Name: |
|
Richard Lowenthal, M.S., MBA |
|
|
|
|
Title: |
|
President and Chief Executive Officer |

Exhibit 99.1 neffy Investor Day March 7, 2024

Forward Looking Statements Statements in this presentation that are not
purely historical in nature are “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. Forward-looking statements in this presentation include, without limitation, statements regarding:
ARS Pharma’s plan to file its NDA early in the second quarter of 2024, with an anticipated PDUFA action date and launch of neffy, if approved, in the second half of 2024; the timing of the EMA’s decision and submissions to other foreign
regulatory authorities; the potential market, demand and expansion opportunities for neffy; ARS Pharma’s expected competitive position; whether the results will be sufficient to demonstrate that neffy is at least as effective as injectable
epinephrine; the timelines for potential regulatory filings, approvals and commercialization of neffy in ex-US regions; ARS Pharma’s marketing and commercialization strategies, including potential partnerships in foreign jurisdictions;
potential benefits of neffy, if approved, including the likelihood that doctors will prescribe neffy and that allergy patients and caregivers will choose to carry and dose neffy compared to needle-bearing options; the expectation of neffy attaining
coverage, including without restriction for 80% of commercial lives within a year of launch; ARS Pharma’s anticipated cash, cash equivalents and short-term investments on hand upon any future approval and launch of neffy; the expected size,
composition and reach of ARS Pharma’s sales force; the availability and functionality of neffyExperience and neffyConnect; the anticipated pricing and co-pay buydown; the anticipated timing and costs of future studies and commercialization
efforts, and their impact on operating runway; ARS Pharma’s projected operating runway; expected intellectual property protection; and any statements of assumptions underlying any of the foregoing. These forward-looking statements are subject
to the safe harbor provisions under the Private Securities Litigation Reform Act of 1995. Because such statements are subject to risks and uncertainties, actual results may differ materially from those expressed or implied by such forward-looking
statements. Words such as “anticipate,” “could,” “demonstrate,” “expect,” “indicate,” “may,” “plan,” “potential,” “will” and similar
expressions are intended to identify forward-looking statements. These forward-looking statements are based upon ARS Pharma’s current expectations and involve assumptions that may never materialize or may prove to be incorrect. Actual results
and the timing of events could differ materially from those anticipated in such forward-looking statements as a result of various risks and uncertainties, which include, without limitation: the PDUFA target action date may be further delayed due to
various factors outside ARS Pharma’s control; the ability to obtain and maintain regulatory approval for neffy; the results of the new clinical trial may not support the approval of neffy; results from clinical trials may not be indicative of
results that may be observed in the future; potential safety and other complications from neffy; the labelling for neffy, if approved; the scope, progress and expansion of developing and commercializing neffy; potential for payers to delay, limit,
or deny coverage for neffy; the size and growth of the market therefor and the rate and degree of market acceptance thereof vis-à-vis intramuscular injectable products; ARS Pharma’s ability to protect its intellectual property position;
uncertainties related to capital requirements; and the impact of government laws and regulations. Additional risks and uncertainties that could cause actual outcomes and results to differ materially from those contemplated by the forward-looking
statements are included under the caption “Risk Factors” in ARS Pharma’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2023, filed with the Securities and Exchange Commission (“SEC”) on November 9,
2023. This and other documents ARS Pharma files with the SEC can also be accessed on ARS Pharma’s website at ir.ars-pharma.com by clicking on the link “Financials & Filings” under the “Investors & Media” tab.
The forward-looking statements included in this presentation are made only as of the date hereof. ARS Pharma assumes no obligation and does not intend to update these forward-looking statements, except as required by law.

Today’s Speakers ARS Management Key Opinion Leaders Richard
Lowenthal, M.S., MSEL Jonathan Spergel, M.D., Ph.D. Chief Executive Officer, Co-Founder Chief of Allergy Program Led FDA approvals for multiple Children’s Hospital of Philadelphia nasal spray products 25+ years of experience Eric Karas Thomas
B. Casale, M.D. Chief Commercial Officer ® Professor of Medicine & Pediatrics Led Narcan commercial ops at Chief, Allergy & Immunology Emergent/Adapt, and Auxilium specialty University of South Florida 25+ years of experience
3
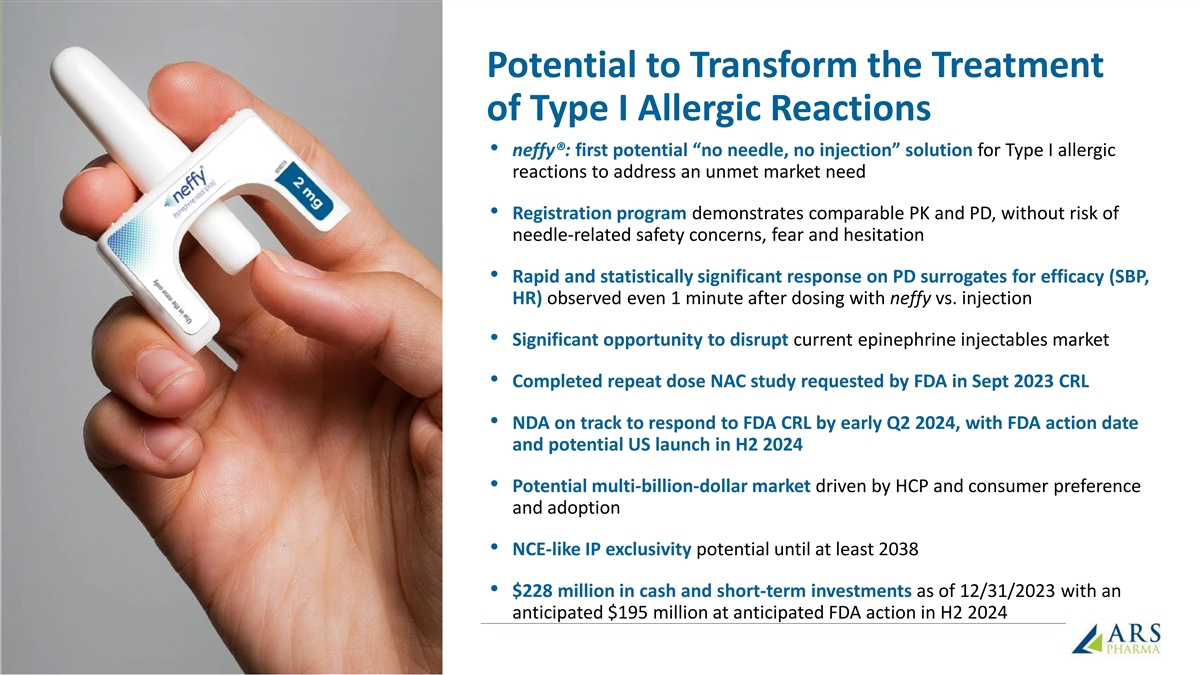
Potential to Transform the Treatment of Type I Allergic Reactions
• neffy®: first potential “no needle, no injection” solution for Type I allergic reactions to address an unmet market need • Registration program demonstrates comparable PK and PD, without risk of needle-related safety
concerns, fear and hesitation • Rapid and statistically significant response on PD surrogates for efficacy (SBP, HR) observed even 1 minute after dosing with neffy vs. injection • Significant opportunity to disrupt current epinephrine
injectables market • Completed repeat dose NAC study requested by FDA in Sept 2023 CRL • NDA on track to respond to FDA CRL by early Q2 2024, with FDA action date and potential US launch in H2 2024 • Potential multi-billion-dollar
market driven by HCP and consumer preference and adoption • NCE-like IP exclusivity potential until at least 2038 • $228 million in cash and short-term investments as of 12/31/2023 with an anticipated $195 million at anticipated FDA
action in H2 2024 4
What We Will Cover Today Unmet need in type I allergic reactions
including anaphylaxis Dr. Jonathan Spergel neffy clinical profile, registrational studies Richard Lowenthal neffy benefit-risk for type I allergic reactions including anaphylaxis Dr. Thomas Casale US market opportunity and commercialization strategy
Eric Karas 5

Unmet Need / Current Challenges Vast Majority of Type I Allergy Patients
Face Significant Limitations with Current Treatment Options NO TREATMENT REFUSAL OF DELAY IN USER ERROR PROBLEM AVAILABLE TREATMENT TREATMENT IN TREATMENT ONLY 10% - 20% of 1 ~40% - 60% of ~50% of patients carry ~25% - 60% do not 23% - 35% fail to
patients with active 2 7 (<20% carry two) , 1,3 5, 6 4 Rx use as indicated patients delay administer dose correctly EASIER AND MORE RELIABLE neffy NO NEEDLE SMALL CONSISTENT DOSING SOLUTIONS NO INJECTION • 99.999% delivery of • Fits
in your pocket; effective dose in can carry more than 1 • Rapid administration • 0% critical dosing errors reliability testing; no without a needle in registration • ~10% of cases require inhalation required self-administration
study repeat doses of • No risk of needle-related 2 1 • 24 month shelf-life at injuries; lacerations or epinephrine • High bioavailability, low 2 room temperature, with cardiotoxic blood vessel mg dose of neffy achieves up to 3
months at high injections comparable PK without o temperatures (122 F) overexposure risk • Less hesitation to dose 6 References: 1. Warren CM, et al. Ann Allergy Asthma Immunol. 2018. 2. Rooney E, et al. Poster Presentation at ACAAI 2022
(Louisville, KY). 3. Brooks C, et al. Ann Allergy Asthma Immunol. 2017. 4. El Turki A, et al. Emerg Med J. 2017. 5. Asthma and Allergy Foundation of American Patient Survey Report 2019. 6. Mehta GD, et al. Expert Rev Clin Immunol. 2023. 7. ARS
company estimates based on IQVIA data and references 1 through 6.

Significant Catalysts for neffy in 2024 o US NDA response to CRL by
early Q2 2024 FDA o PDUFA action date anticipated in H2 2024 o EMA decision (CHMP Opinion) expected by mid-2024 EMA o China NDA filing expected by YE 2024 o Japan NDA filing expected by YE 2024 o Planning in progress for filing in other major ex-US
regions including Canada o Expansion opportunities • Positive data from Phase 2 chronic urticaria study reported in Feb 2024 • Initiation of Phase 2b outpatient urticaria study 7
Type I Allergies & Unmet Needs Jonathan M. Spergel, M.D., Ph.D.
Professor of Pediatrics Chief of the Allergy Program Children’s Hospital of Philadelphia

Type I Allergic Reactions: Systemic Hypersensitivity Reaction More than
500,000 ER visits ~40 Million people in each year due to systemic Type I allergic US with systemic Type I allergic 1 2 reactions , costing an average of $1600+ per visit reaction to allergens Other Type I allergy indications Significant
co-morbidities and symptomatic Caused by exposure to a specific allergen, (e.g. urticaria flares) impact on quality of life. most commonly food, venom, drugs References: 1. Carillo-Martin I, et al. J Allergy Clin Immunol Pract 2020. 2. BlueCross
BlueShield of America. Childhood Allergies in America 2018 9 Images reproduced with permission

Mucosal Respiratory Cardiac GI Anaphylaxis Diagnosis Criteria and
Symptoms 2-14 Symptoms (>2%) reported during US anaphylaxis events 0% 20% 40% 60% 80% 100% Urticaria or Angioedema Urticaria Flushing Pruritus Angioedema (e.g. face, lips, tongue or larynx) Intraoral Edema or Tongue Swelling Laryngeal Edema
Throat pruritus Orophyarngeal Edema Difficulty Breathing / Dyspnea Throat Tightness Wheezing Bronchospasm Hoarseness Cough Chest tightness / Chest pain Respiratory failure Stridor Nasal symptoms / rhinitis Tachycardia Presyncope / Dizziness /Light
headedness Hypotension Confusion/somnolence Loss of consciousness Dysphagia Vomiting / Emesis Diarrhea + Abdominal Pain Nausea Abdominal pain or cramping Diarrhea References: 1. Shaker MS, et al. J Allergy Clin Immunol. 2020. 2. Pistiner M, et al. J
Allergy Clin Immunol Pract. 2021. 3. Jalil M, et al. Abstract at AAAAI 2020 Virtual Meeting. 4. Gonzelez-Estrada A, et al. Ann Allergy Asthma Immunol. 10 2018. 5. Lee S, et al. J Allergy Clin Immunol. 2017. 6. Lee S, et al. J Allergy Clin Immunol
Pract. 2014. 7. Manivannan V, et al. Am J Emerg Med. 2014. 8. Wood RA, et al. J Allergy Clin Immunol 2014. 9. Walsh KE, et al. Pharmacoepidemiol Drug Saf 2013. 10. Decker WW, et al. J Allergy Clin Immunol. 2008. 11. Ross MP, et al. J Allergy Clin
Immunol. 2008. 12. Webb LM & Lieberman P. Ann Allergy Asthma Immunol. 2006. 13. Ditto AM, et al. Ann Allergy Asthma Immunol. 1996. 14. Rudders SA, et al. Pediatrics. 2010. Note that some publications do not specify angioedema symptom subtype.
Angioedema subtype frequency aggregated when reported.

Most frequently reported symptoms are difficulty breathing, angioedema
(face, lips, tongue, larynx) and urticaria (hives) References: 1. LoVerde D, et al. Chest. 2018. 2. Images reproduced with permission 11

Epinephrine: Well Known Mechanism of Action Adrenergic Pharmacological
Effect Clinical Effect Receptor of Epinephrine of Epinephrine • Stabilizes mast cells and basophils - • Reverses pathological histamine cascade Inhibits inflammatory mediators • Increase in bronchial airflow β 2 •
Relaxation of bronchial smooth muscles • Increases blood to skeletal muscle • Vasodilation in skeletal vasculature β • Increases blood pressure and heart rate • Relieves hypotension and shock 1 • Increases systolic
blood pressure • Relieves hypotension and shock • Causes blood vessel constriction α 1 • Relieves upper airway obstruction • Decreases mucosal edema Receptor Sensitivity 12
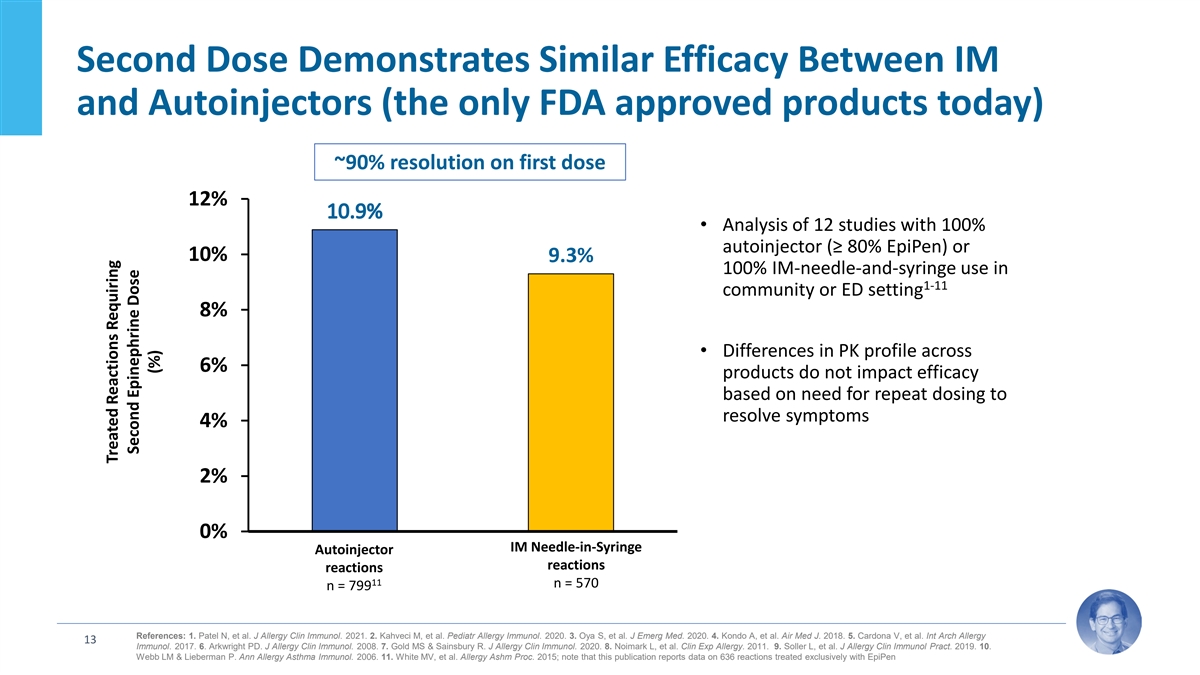
Second Dose Demonstrates Similar Efficacy Between IM and Autoinjectors
(the only FDA approved products today) ~90% resolution on first dose 12% • Analysis of 12 studies with 100% autoinjector (≥ 80% EpiPen) or 10% 9.3% 100% IM-needle-and-syringe use in 1-11 community or ED setting 8% • Differences in
PK profile across 6% products do not impact efficacy based on need for repeat dosing to resolve symptoms 4% 2% 0% IM Needle-in-Syringe Autoinjector % r equiring second dose reactions reactions 11 n = 570 n = 799 References: 1. Patel N, et al. J
Allergy Clin Immunol. 2021. 2. Kahveci M, et al. Pediatr Allergy Immunol. 2020. 3. Oya S, et al. J Emerg Med. 2020. 4. Kondo A, et al. Air Med J. 2018. 5. Cardona V, et al. Int Arch Allergy 13 Immunol. 2017. 6. Arkwright PD. J Allergy Clin Immunol.
2008. 7. Gold MS & Sainsbury R. J Allergy Clin Immunol. 2020. 8. Noimark L, et al. Clin Exp Allergy. 2011. 9. Soller L, et al. J Allergy Clin Immunol Pract. 2019. 10. Webb LM & Lieberman P. Ann Allergy Asthma Immunol. 2006. 11. White MV, et
al. Allergy Ashm Proc. 2015; note that this publication reports data on 636 reactions treated exclusively with EpiPen Treated Reactions Requiring Second Epinephrine Dose (%)
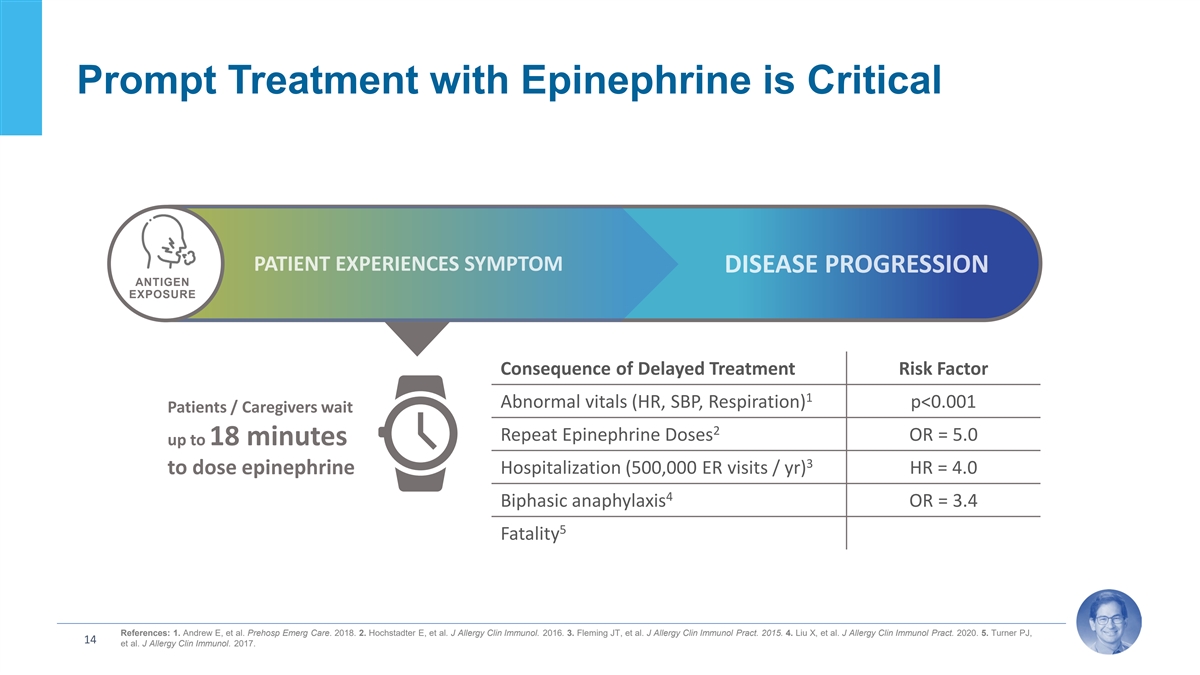
Prompt Treatment with Epinephrine is Critical ANTIGEN EXPOSURE
Consequence of Delayed Treatment Risk Factor 1 Abnormal vitals (HR, SBP, Respiration) p<0.001 Patients / Caregivers wait 2 Repeat Epinephrine Doses OR = 5.0 up to 18 minutes 3 Hospitalization (500,000 ER visits / yr) HR = 4.0 to dose epinephrine
4 Biphasic anaphylaxis OR = 3.4 5 Fatality References: 1. Andrew E, et al. Prehosp Emerg Care. 2018. 2. Hochstadter E, et al. J Allergy Clin Immunol. 2016. 3. Fleming JT, et al. J Allergy Clin Immunol Pract. 2015. 4. Liu X, et al. J Allergy Clin
Immunol Pract. 2020. 5. Turner PJ, 14 et al. J Allergy Clin Immunol. 2017.
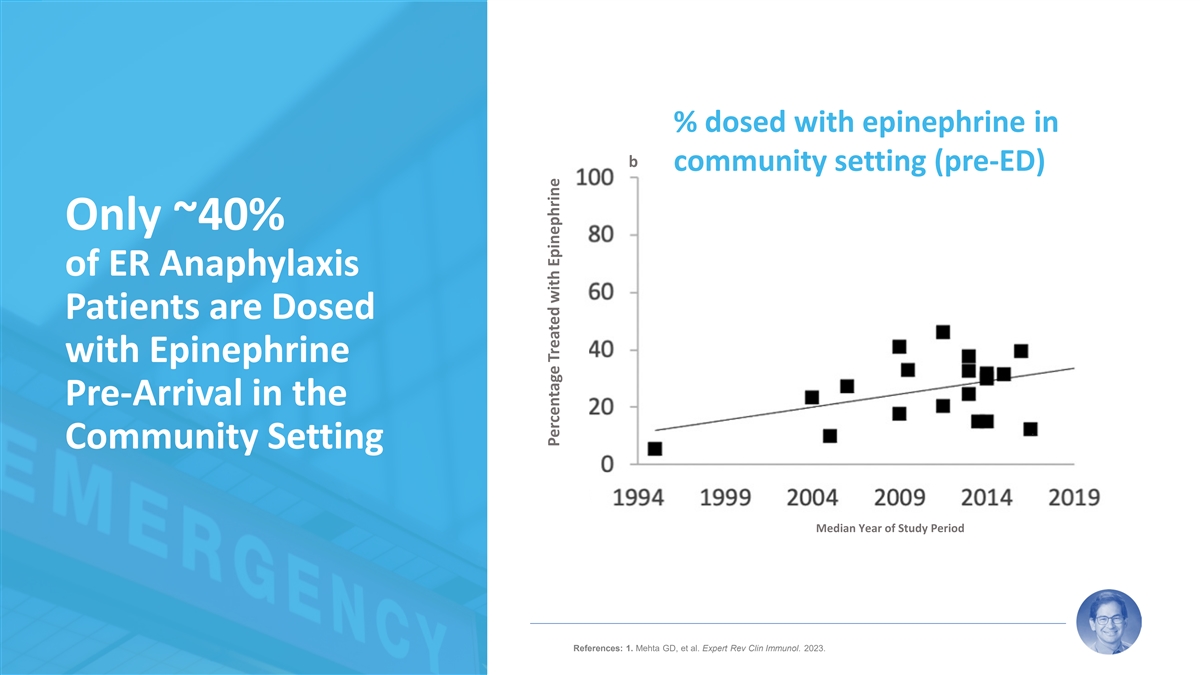
% dosed with epinephrine in b community setting (pre-ED) Only ~40% of
ER Anaphylaxis Patients are Dosed with Epinephrine Pre-Arrival in the Community Setting Median Year of Study Period 15 References: 1. Mehta GD, et al. Expert Rev Clin Immunol. 2023. Percentage Treated with Epinephrine

Delays in Treatment with Epinephrine are Principally Due to
Autoinjector Limitations and Accompanying Patient Reluctance ~40% of patients do not >40% of patients do not fill or refill 40% 2 1 40% administer epinephrine at all their epinephrine prescription >50% of parents are afraid or 55%-60%
don’t consistently somewhat afraid to administer 50% 2-4 60% carry epinephrine 5 their child’s epinephrine ~20% of patients Patients that Do Not ~70% of patients 20% 70% with Training Without Training 7 Administer Correctly References:
1. Data on File. ARS Pharmaceuticals. 2023. 2. Warren CM, et al. Ann Allergy Asthma Immunol. 2018. 3. Brooks C, et al. Ann Allergy Asthma Immunol. 2017. 4. Curtis C, et al. Ann Allergy Asthma Immunol. 2014. 5. Chad L, 16 et al. Eur J Allergy Clin
Immunol. 2013. 6. Sicherer SH, et al. Pediatrics. 2000. 7. El Turki A, et al. Emerg Med J. 2017.

Needle-Related Safety Risks & Use Errors Needle-related risks
defined in labeling for all autoinjectors Ø Lacerations and bone injections Ø IV bolus injection (blood vessel injections) – likely result in most serious AEs Accidental self-injection into extremity by patient or caregiver 1 Ø
~ 3,500 events per year reported Ø Requires immediate medical attention (treatment in ER typical) 2 Injection site pain, infection and other reactions Wet injections (withdraw needle too quickly) and other dosing errors 3,4,5,6,7,8,9 User
errors and device malfunctions References: 1. Anshien M, et al. Am J Ther. 2019. 2. Guerlain S, et al. Ann Allergy Asthma Immunol. 2011. 3. El Turki A, et al. Emerg Med J. 2017. 4. Moss RB, et al. Ann Allergy Asthma Immunol. 2018. 5. 17 Sanofi.
Auvi-Q Recall. October 2015. 6. FDA. EpiPen and EpiPen Jr Recall. March 2017. 7. FDA. EpiPen auto-injector errors related to device malfunctions and user administration. March 2020. 8. FDA. Amneal and Impax Laboratories epinephrine auto-injector
device malfunctions. June 2020. 9. FDA. Recall of Symjepi (epinephrine) injection for potential manufacturing defect. March 2022.

2023 AAAAI guidelines updated so that EMS activation not required for
90% of events that resolve with single dose Historic guidelines recommended ED visit following use of epinephrine for anaphylaxis, which may result in families not giving epinephrine to avoid ED visits Based on outcomes of anaphylaxis in EDs and the
COVID-19 pandemic, data indicates treatment and monitoring of anaphylaxis can occur at home Ø If signs and symptoms resolve within minutes of dosing, monitor at home after first dose Ø If signs and symptoms improve within minutes of
dosing, monitor at home if comfortable, while considering EMS activation and possible second dose of epinephrine Ø If signs and symptoms are not resolving, activate EMS immediately, and consider second dose of epinephrine Prompt use of
epinephrine and monitoring at home will decrease healthcare utilization 18

neffy (epinephrine nasal spray) Can Fill Great Unmet Medical Need for
Patients and Caregivers Epinephrine has a well-established efficacy and safety profile Ø Efficacy same across epinephrine injection products despite PK differences Immediate administration of epinephrine is critical Patients and caregivers
reluctant to use or carry current devices Ø Needle-phobia Ø Concerns with safety Ø Cumbersome to carry Unmet need for needle-free, easy to use, easy to carry, safe and effective epinephrine option neffy can fit that need for our
patients 19

neffy Profile Richard Lowenthal CEO, ARS Pharma

neffy is a High Bioavailability, Low 2 mg Dose Saline-Based Nasal
Spray: Proven Triad of FDA-Approved Components High bioavailability with low dose minimizes side effects that mimic anaphylaxis (GI symptoms) > 9 FDA Approvals in Allergy and risk of cardiotoxicity from overdosing (> 100 years of clinical
experience) Epinephrine 7 FDA Approvals of Sprayer 1 (> 55 million Rx, 99.999% reliable) 3 FDA Approvals incl. Intravail 1 (> 1 million Rx) ® ® ® NARCAN VALTOCO NAYZILAM ® ® ® TOSYMRA VALTOCO Intravail Sprayer
® ® ® ZAVZPRET dodecyl-maltoside: IMITREX TOSYMRA GRAS absorption enhancer ® OPVEE ® OPVEE 21 References: 1. IQVIA Prescription data, and ARS company data on file

Intravail® Allows Injection-Like PK at a Low Intranasal Dose
Without Irritation or Pain, and Robust IP Protection to 2038+ NCE-like exclusivity enabled by Intravail • No systemic absorption via nose without Intravail when epinephrine is put in water-based solution • Intravail allows systemic
intranasal absorption of epinephrine within the known therapeutic dose window for n-Dodecyl beta-D-maltoside (Intravail®) injection products • Generally recognized as safe (GRAS) absorption • No inhalation required –
absorption in nasal mucosa enhancing agent • Issued composition of matter patents in the US and • Biologic surfactant that loosens tight junctions ® 1, 2 globally covering Intravail + epinephrine (paracellular) coupled with
fluidization and • Issued method of treatment patents blocks other low dose penetration of cell membranes (transcellular) 3-7 aqueous nasal sprays (<4 mg dose) • No irritation, pain or damage to nasal mucosa • Extensive
toxicology and safety program • Exclusivity until at least 2038 without PTE References: 1. US10,576,156, 2. US11,173,209, 3. US10,682,414, 4. US11,191,838, 5. US11,744,895, 6. US11,717,571, 7. US11,918,655 22

Designed for Easier Carry and Portability 23 Case holds two neffy 2mg
devices.
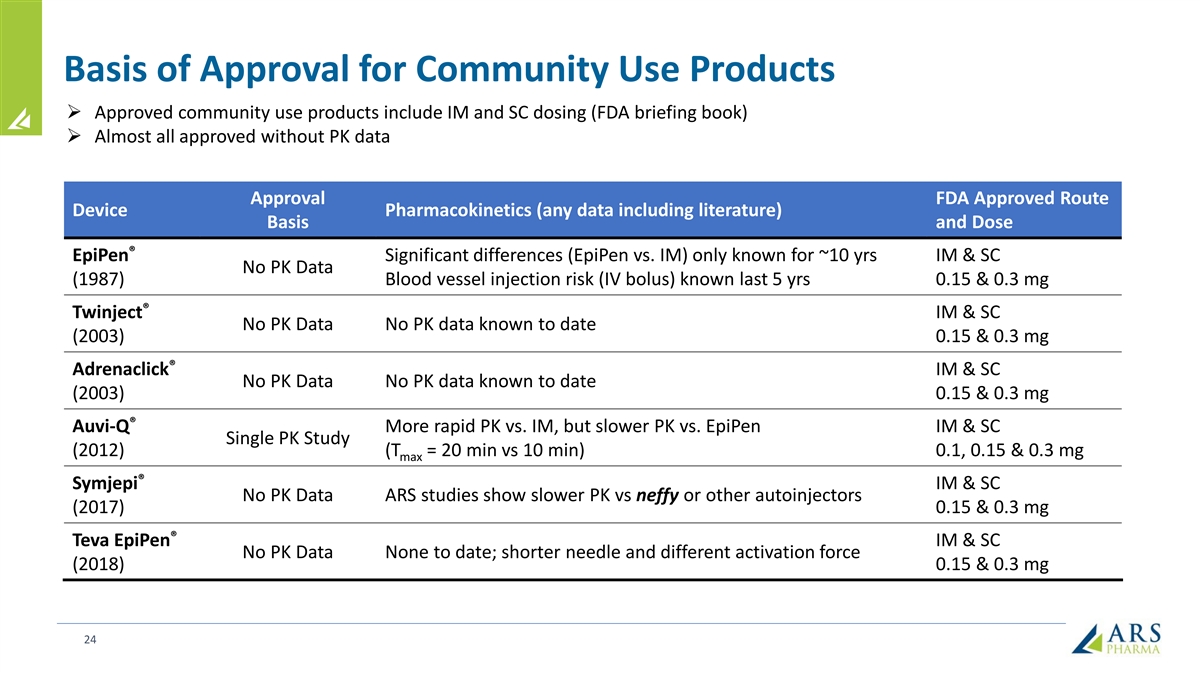
Basis of Approval for Community Use Products Ø Approved community
use products include IM and SC dosing (FDA briefing book) Ø Almost all approved without PK data Approval FDA Approved Route Device Pharmacokinetics (any data including literature) Basis and Dose ® EpiPen Significant differences (EpiPen vs.
IM) only known for ~10 yrs IM & SC No PK Data (1987) Blood vessel injection risk (IV bolus) known last 5 yrs 0.15 & 0.3 mg ® Twinject IM & SC No PK Data No PK data known to date (2003) 0.15 & 0.3 mg ® Adrenaclick IM &
SC No PK Data No PK data known to date (2003) 0.15 & 0.3 mg ® Auvi-Q More rapid PK vs. IM, but slower PK vs. EpiPen IM & SC Single PK Study (2012) (T = 20 min vs 10 min) 0.1, 0.15 & 0.3 mg max ® Symjepi IM & SC No PK Data
ARS studies show slower PK vs neffy or other autoinjectors (2017) 0.15 & 0.3 mg ® Teva EpiPen IM & SC No PK Data None to date; shorter needle and different activation force (2018) 0.15 & 0.3 mg 24

All Products Demonstrate Efficacy Despite Different PK Ø Despite
PK differences no known difference in efficacy Ø All products 90% resolution on single dose Median or Mean Mean Study C Study T Range 1 max max Treatment Source N Study T max (pg/mL) (min) (min) EpiPen 0.3 mg Literature and ARS 507 288 –
869 5 to 40 1 – 240 IM 0.3 mg Literature and ARS 381 209 – 489 30 to 60 3 – 360 Auvi-Q 0.3 mg Literature 96 486 – 646 20 to 30 5 – 60 Symjepi 0.3 mg ARS data 88 337 – 438 30 4 – 240 SC 0.3 mg ARS 36 246 45 4
– 180 Total Range 209 to 869 5 to 60 1 to 360 References: 1. Srisiwat C, et al. Asian Pac J Allergy Immunol. 2022. 2. Aquestive Therapeutics Press Release. Sept 2022. 3. Edwards ES, et al. Ann Allergy Asthma Immunol. 2013. 4. Dworaczyk D &
Hunt A. Abstract Presentation 25 AAAAI 2021 (Virtual Meeting). 5. Aquestive Therapeutics Press Release. May 2023.

Development Program Focused on Comparison to PK / PD Profile of
Approved Epinephrine Products PK to ensure efficacious and safe exposures PD response to support effect at achieving within range of approved products - receptor response Bracketing Approach • Blood pressure (BP): α & β (β )
receptors 1 1 2 • Minimum exposure ≥ IM/SC (efficacy) • Heart rate (HR): β receptors 1 • Maximum exposures < EpiPen (safety) 26
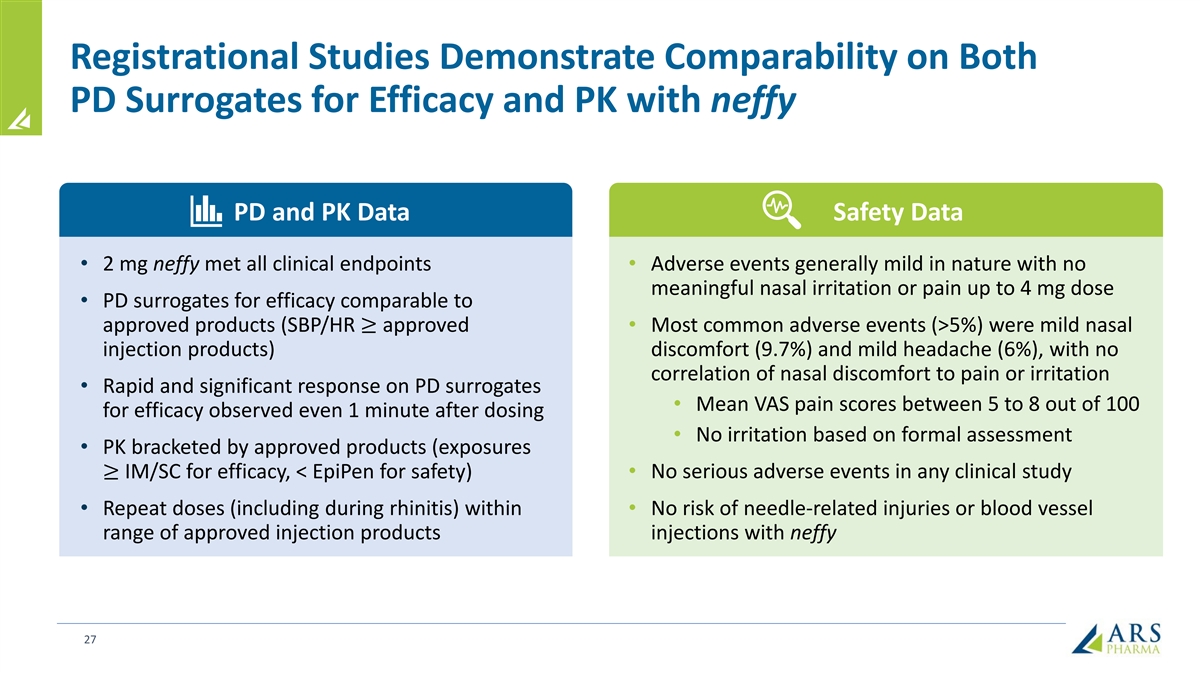
Registrational Studies Demonstrate Comparability on Both PD Surrogates
for Efficacy and PK with neffy PD and PK Data Safety Data • 2 mg neffy met all clinical endpoints • Adverse events generally mild in nature with no meaningful nasal irritation or pain up to 4 mg dose • PD surrogates for efficacy
comparable to approved products (SBP/HR ≥ approved • Most common adverse events (>5%) were mild nasal injection products) discomfort (9.7%) and mild headache (6%), with no correlation of nasal discomfort to pain or irritation •
Rapid and significant response on PD surrogates • Mean VAS pain scores between 5 to 8 out of 100 for efficacy observed even 1 minute after dosing • No irritation based on formal assessment • PK bracketed by approved products
(exposures ≥ IM/SC for efficacy, < EpiPen for safety) • No serious adverse events in any clinical study • Repeat doses (including during rhinitis) within • No risk of needle-related injuries or blood vessel range of
approved injection products injections with neffy 27

Pharmacokinetic Results from neffy 2 mg Studies Satisfies Bracketing
Approach designed with FDA 450 neffy 2.0 mg (HCP) (n=78)* 400 neffy 2.0 mg (self-administration) (n=42) Upper bracket for safety 350 IM 0.3 mg (n=178) EpiPen 0.3 mg (n=77) 300 SC 0.3 mg (n=35) 250 Lower bracket for efficacy 200 150 100 50 0 0 30 60
90 120 150 180 210 240 270 300 330 360 Time (Minutes) *Includes Studies EPI-15 and EPI-16 28 Mean Epinephrine Concentration (pg/mL)

neffy PK is Bracketed by EpiPen Studies (Cmax or tmax) Mean Study C
Median Study T max max Treatment Study Reference N (pg/mL) (min) AQST-109 EPIPHAST II Results (2022) 22 869 22 ARS EPI-JP01 Data (2020) 30 676 10 AQST-109 Pilot Results (2023) 27 628 10 ARS EPI-15 (2022) 35 612 8 Tal et al. EAACI (2022) 12 550 9
EpiPen (0.3 mg) ARS EPI-11b Data (2021) 9 537 6 Edwards et al. NDA #201739 (2012) 67 520 10.2 Chen et al. AAAAI (2019) 11 511 5 ARS EPI-12 Data (2021) 36 493 8 ARS EPI-13 Data (2022) 39 490 6 ARS EPI-16 data (2022) 36 491 20 ARS integrated analysis
(2022) – EPI-15/16 78 485 20.5 neffy (2.0 mg) ARS EPI-15 data (2022) 42 481 30 ARS EPI-17 data (2022) 42 421 30 Worm et al. Clin Transl Allergy (2020) 12 390 to 530 9 to 30 Turner et al. Clin Exp Allergy (2021) 37 386 40 Amphastar
US2021/030502 (2021) 56 364 - 458 7-15 ARS EPI-07 Data (2019) 35 375 24 Dworaczyk et al. AAAAI (2020) 55 308 to 440 10-16 EpiPen (0.3 mg) Oppenheimer et al. AAAAI (2022) 10 341 22 ARS EPI-01 Data (2018) 12 333 20 Aquestive R&D Day (2021) 9 300
10 Dworaczyk et al. AAAAI (2021) 25 288 10 Dworaczyk et al. ACAAI (2023) 26 279 20 Dworaczyk et al. ACAAI (2023) 25 228 21 29
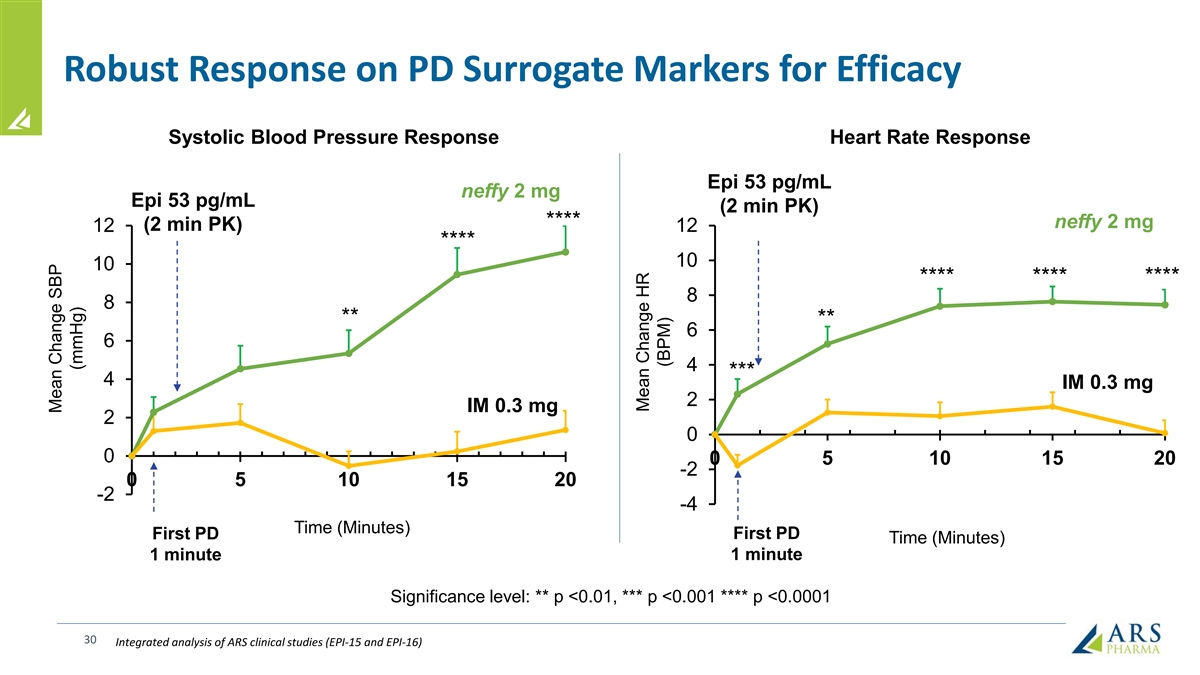
Robust Response on PD Surrogate Markers for Efficacy Systolic Blood
Pressure Response Heart Rate Response Epi 53 pg/mL neffy 2 mg Epi 53 pg/mL (2 min PK) **** neffy 2 mg (2 min PK) 12 12 **** 10 10 **** **** **** 8 8 ** ** 6 6 4 *** 4 IM 0.3 mg 2 IM 0.3 mg 2 0 0 0 5 10 15 20 -2 0 5 10 15 20 -2 -4 Time (Minutes)
First PD First PD Time (Minutes) 1 minute 1 minute Significance level: ** p <0.01, *** p <0.001 **** p <0.0001 30 Integrated analysis of ARS clinical studies (EPI-15 and EPI-16) Mean Change SBP (mmHg) Mean Change HR (BPM)
Positive FDA AdCom vote supports benefit-risk of neffy FDA Advisory
Committee (May 2023) voted that benefit-risk of neffy supported FDA approval Ø 17:5 and 16:6 voted in favor for approval in pediatric and adult populations, respectively Ø Advisory members who voted against approval desired comparative
clinical efficacy data for anaphylaxis, which cannot be ethically conducted in this population FDA Advisory Committee viewed single dose NAC study data as “encouraging” and “favorable” due to greater concentration levels
during the period when clinical response is observed with epinephrine Ø Nasal congestion following nasal-allergen challenge (spraying purified antigen directly into the nose) accelerates absorption of neffy in the first 20 minutes vs. normal
state Ø Treatment guidelines recommend giving a second dose if no response is observed within 5 to 15 minutes of administration Ø FDA reported that the rate of nasal mucosal symptoms in anaphylaxis patients ranges from 2 to 11% (weighted
average frequency in the literature is ~4% based on aggregated analysis of 13 publications) No member of the Advisory Committee requested a repeat dose rhinitis study as a prerequisite for FDA approval 31

Completion of Repeat Dose neffy NAC study per FDA’s CRL Request
Shows PK/PD Greater or Similar to IM Injection PD Response (Mean Change in SBP, HR) PK Profile (Mean Plasma Concentrations, pg/mL) neffy 2 mg twice (R/L) Normal (N=42) Mean Change in SBP (mmHg) Mean Change in HR (bpm) IM epinephrine 0.3 mg twice
(R/L) Normal (N=42) neffy 2 mg twice (R/L) NA C (N=40) 16 20 neffy 2 mg twice (R/R) NA C (N=41) 900 IM epinephrine 0.3 mg twice (R/L) NA C (N=42) 18 14 16 800 12 700 14 10 600 12 8 500 10 400 8 6 300 6 4 200 4 2 100 2 0 0 0 0 15 30 45 60 0 30 60 0
30 60 -2 Time (minutes) Time (minutes) Time (minutes) Response to FDA’s CRL anticipated by early Q2 2024 followed by up to 6-month FDA review 32 Note: FDA explicitly requested IM epinephrine as the comparator in this study because IM is the
basis for efficacy for epinephrine products, and there are no known differences between the various approved injection devices despite different PK

Risk-benefit assessment of neffy Thomas B. Casale, M.D. Professor of
Medicine & Pediatrics Chief, Allergy & Immunology University of South Florida

Ideal Properties of an Epinephrine Delivery Product Does it work? Is it
safe? Will patients use it? Ø Consistent and reproducible PK/PD Ø No risk of injury and Ø Minimal side effects profiles (no to minimal outliers) and minimal side effects drug administration that is not Ø Palatable affected by
anaphylaxis symptoms Ø Minimize risk of overdosing Ø Small or pre-existing conditions or co- with epinephrine morbidities Ø Easy to use Ø Avoid side effects that are Ø Robust and rapid PD effects that are also anaphylaxis
symptoms especially important for severe anaphylaxis 34
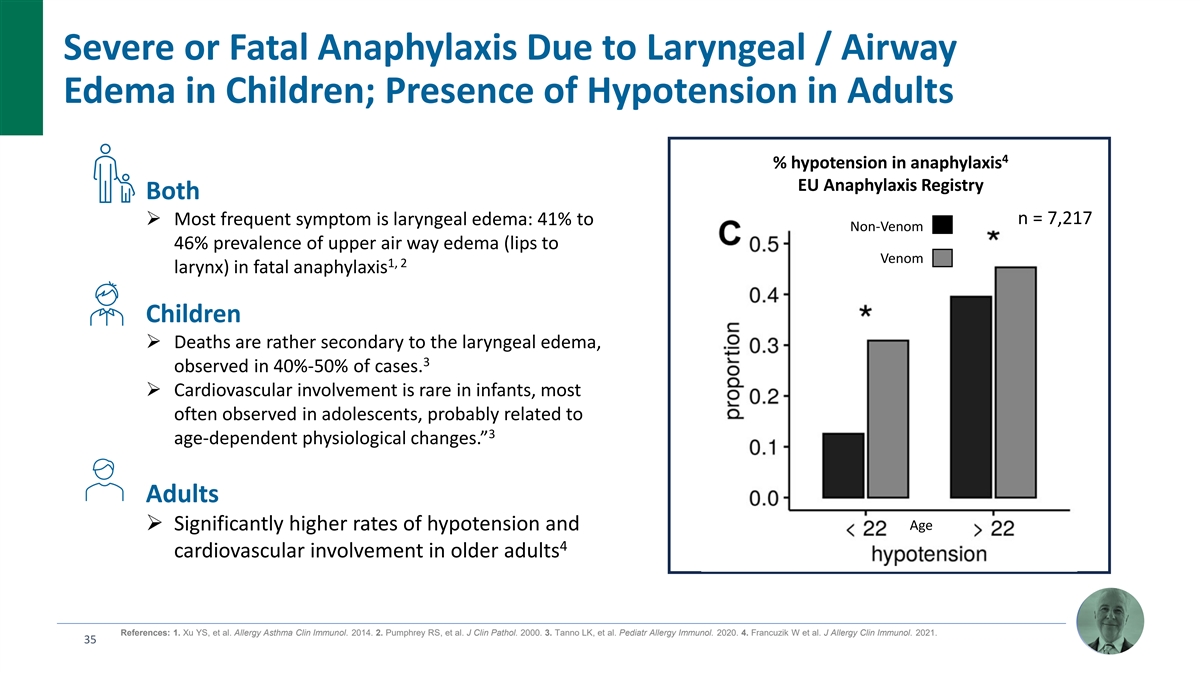
Severe or Fatal Anaphylaxis Due to Laryngeal / Airway Edema in
Children; Presence of Hypotension in Adults 4 % hypotension in anaphylaxis EU Anaphylaxis Registry Both n = 7,217 Ø Most frequent symptom is laryngeal edema: 41% to Non-Venom 46% prevalence of upper air way edema (lips to Venom 1, 2 larynx) in
fatal anaphylaxis Children Ø Deaths are rather secondary to the laryngeal edema, 3 observed in 40%-50% of cases. Ø Cardiovascular involvement is rare in infants, most often observed in adolescents, probably related to 3 age-dependent
physiological changes.” Adults Age Ø Significantly higher rates of hypotension and 4 cardiovascular involvement in older adults References: 1. Xu YS, et al. Allergy Asthma Clin Immunol. 2014. 2. Pumphrey RS, et al. J Clin Pathol. 2000. 3.
Tanno LK, et al. Pediatr Allergy Immunol. 2020. 4. Francuzik W et al. J Allergy Clin Immunol. 2021. 35

neffy Shows Rapid and Robust PD Response that Demonstrates Engagement
of Receptors that Reverse Anaphylaxis Symptoms Systolic Blood Pressure Response Heart Rate Response neffy 2 mg Epi 53 pg/mL Epi 53 pg/mL (2 min PK) (2 min PK) **** neffy 2 mg 12 12 **** 10 10 **** **** **** 8 8 ** ** 6 6 4 *** 4 IM 0.3 mg 2 IM 0.3
mg 2 0 0 0 5 10 15 20 -2 0 5 10 15 20 -2 -4 Time (Minutes) Time (Minutes) First PD First PD 1 minute 1 minute Significance level: ** p <0.01, *** p <0.001 **** p <0.0001 36 Integrated analysis of ARS clinical studies (EPI-15 and EPI-16)
Mean Change SBP (mmHg) Mean Change HR (BPM)
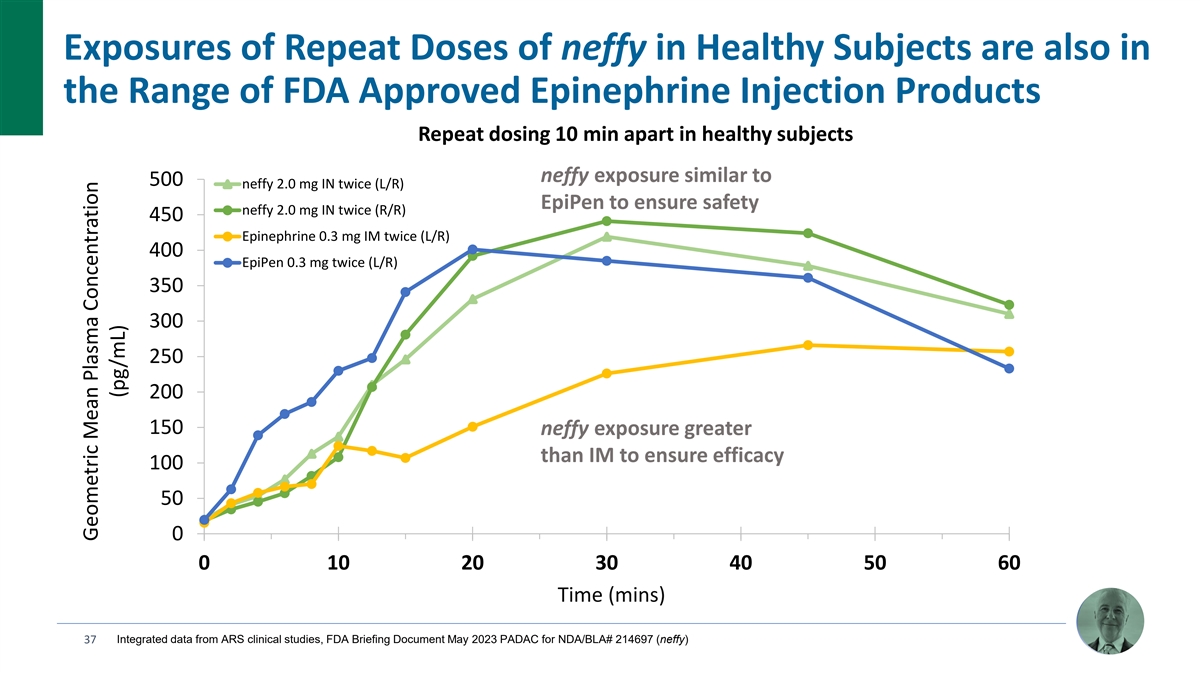
Exposures of Repeat Doses of neffy in Healthy Subjects are also in the
Range of FDA Approved Epinephrine Injection Products Repeat dosing 10 min apart in healthy subjects neffy exposure similar to 500 neffy 2.0 mg IN twice (L/R) EpiPen to ensure safety neffy 2.0 mg IN twice (R/R) 450 Epinephrine 0.3 mg IM twice (L/R)
400 EpiPen 0.3 mg twice (L/R) 350 300 250 200 1.65x 150 neffy exposure greater than IM to ensure efficacy 100 50 0 0 10 20 30 40 50 60 Time (mins) 37 Integrated data from ARS clinical studies, FDA Briefing Document May 2023 PADAC for NDA/BLA# 214697
(neffy) Geometric Mean Plasma Concentration (pg/mL)

PD Response as Shown to be at Least as Good as EpiPen, Supporting
Engagement of Receptors that Reverse Anaphylaxis Symptoms Single Dose SBP Response Twice Dose SBP Response p = 0.947 (ns) 75 p < 0.0001 55 65 45 55 Mean: Mean: 35 Mean: 45 Mean: 22.3 mm 28.9 mm Mean: 29.1 … Mean: 18.2 mm Hg Hg 22.6 mm Mean:
13.4 mm Hg 35 25 Hg 11.6 mm E Hg E max max Hg (mmHg) (mmHg) 25 15 15 5 5 -5 p = 0.01 -5 p < 0.0001 p = 0.0787 (ns) -15 -15 2 mg x 2 mg x 0.3 mg 0.3 mg EpiPen neffy IM 2 neffy 2 neffy EpiPen IM 0.3 mg 2 mg 0.3 mg (L/R) (R/R) n = 78 n = 70 n = 77 n
= 78 n = 178 n = 39 n = 39 38

neffy Shows Robust and Rapid Clinical Resolution of Oral Food Challenge
Induced Anaphylaxis Symptoms Efficacy Study of neffy in Oral Food Challenge Study Outcomes 1 Induced Anaphylaxis (EPI-JP-03) Clinical Response Rate (%) Study Design: single arm, open-label study neffy 100.0% Participants: 15 pediatric subjects (aged
6 to 17): (EPI-JP-03) Ø 9 subjects (30 kg+) Ø 6 subjects (15-30 kg) Patients experiencing Grade 2 (moderate) or higher 100% of patients responded to a single dose of neffy 3 anaphylaxis symptoms (out of 3 grade scale) following in the
first 15 minutes, and did not require a second oral food challenge dosed with a single dose of either dose of epinephrine per treatment guidelines 2 mg or 1 mg neffy: Ø Mucosal: generalized urticaria/exanthema/wheal pruritus, 100% of patients
experienced complete resolution of swollen face, throat pain 2 Ø GI: moderate abdominal pain, recurrent emesis/diarrhea, the anaphylaxis symptoms with single dose of neffy Ø Respiratory: repetitive cough, chest tightness/wheezing
detectable via auscultation 16 min median time to complete resolution of Ø Circulatory: pale face/mild hypotension/tachycardia (>15 beats/min), light-headedness/feeling of “pending anaphylaxis following single dose of neffy
doom”/somnolence/headache References: 1. Ebisawa M, et al. Presentation at AAAAI 2024 (Washington DC). 2. 100% of EPI-JP-03 patients dosed with neffy did not require a second dose in the first 15 minutes per guidelines because a response was
not being 39 observed, and 100% of patients achieved complete resolution of symptoms. 1 of the 16 subjects (6.7%) challenged with egg experienced a biphasic reaction 2h 45 min after being dosed with a single dose of neffy and achieving complete
resolution of symptoms. This is consistent with the 12.8% frequency of biphasic reactions reported in children with food-induced anaphylaxis.(Gupta RS, et al. J Allergy Clin Immunol Pract. 2021).
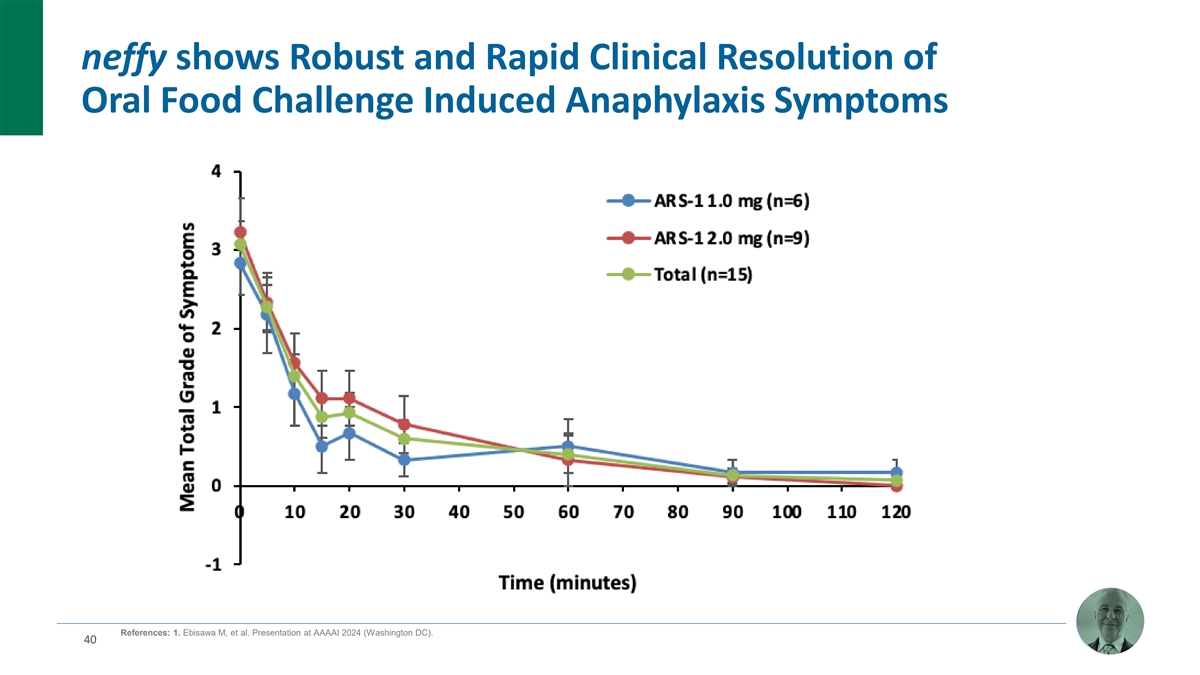
neffy shows Robust and Rapid Clinical Resolution of Oral Food Challenge
Induced Anaphylaxis Symptoms References: 1. Ebisawa M, et al. Presentation at AAAAI 2024 (Washington DC). 40

neffy Shows Robust and Rapid Clinical Responses in Treatment- Resistant
Urticaria (Most Common Symptom of Anaphylaxis) Randomized, Placebo-Controlled Efficacy Data in 1 Treatment Refractory Chronic Urticaria (EPI-U01) Study Design randomized, placebo-controlled crossover trial study • 18 chronic urticaria subjects
who experience flares at least two times a week while on chronic treatment (antihistamines +/- Xolair) • Patients come to clinic when experiencing a flare and are treated with 2 mg, 1 mg or placebo References: 1. Bernstein D, et al.
Presentation at AAAAI 2024 (Washington DC). 41

Experimental NAC-Induced Rhinitis Does Not Negatively Impact
neffy’s PK Profile (Allergic Rhinitis Subjects) FDA Advisory Committee viewed neffy NAC data as “encouraging” and “favorable” Repeat dose under NAC-induced rhinitis supports similarity NAC-induced rhinitis accelerates
absorption of single to injection for more severe cases of anaphylaxis dose neffy, but within the range of injection neffy 2 mg twice (R/L) Normal (N=42) IM epinephrine 0.3 mg twice (R/L) Normal (N=42) Dosing 10 min apart neffy 2.0 mg neffy 2.0 mg
rhinitis ARS-1 2.0 mg IN ARS-1 2.0 mg IN with Rhinitis neffy 2 mg twice (R/L) NA C (N=40) 900 IM 0.3 mg Epinephrine 0.3 mg IM neffy 2 mg twice (R/R) NA C (N=41) 300 800 IM epinephrine 0.3 mg twice (R/L) NA C (N=42) 250 700 600 200 500 * 150 * 400 *
* * * 300 100 200 50 100 0 0 0 10 20 30 40 0 10 20 30 40 Time (minutes) Time (minutes) Time to observe clinical response, Time to observe clinical response, and re-dose per guidelines and re-dose per guidelines 42 * Statistically significant
differences between neffy with rhinitis compared to IM injection (p <0.05) Mean Epinephrine Concentration (pg/mL)

Experimental NAC-Induced Rhinitis Does Not Negatively Impact
neffy’s PD Profile (Repeat Doses 10 min Apart) Mean Change in Heart Rate (bpm) Mean Change in Systolic Blood Pressure (mmHg) neffy 2 mg twice (R/L) Normal (N=42) IM epinephrine 0.3 mg twice (R/L) Normal (N=42) neffy 2 mg twice (R/L) NAC (N=40)
16 neffy 2 mg twice (R/R) NAC (N=41) 20 IM epinephrine 0.3 mg twice (R/L) NAC (N=42) 14 18 16 12 14 10 12 8 10 8 6 6 4 4 2 2 0 0 0 30 60 0 30 60 -2 Time (minutes) Time (minutes) 43

Upper Respiratory Tract Infection (URTI)-Induced Rhinitis has no
Clinically Meaningful Impact on the PK/PD Profile of neffy Mean Epinephrine Plasma Mean Systolic Blood Pressure Change 18 500 n ne ef ff fy y 2.0 mg neffy neffy 2.0 mg neffy neffy 2.0 mg with URTI 16 neffy neffy 2.0 mg with URTI 400 14 12 300 10 8
200 6 4 100 2 0 0 0 20 40 60 80 100 120 0 50 100 150 200 250 -2 Time (Minutes) Time (Minutes) 44 N = 21 URTI / 16 Normal (returned) Mean Epinephrine Concentration (pg / mL) ±SE Mean SBP Change from Baseline (mmHg) ± SE

PK/PD Profile and Ability to Dose May Be Influenced By Varying
Conditions Including Anaphylaxis Itself Headache Cardiac failure/arrest Oral/palatal pruritus/stinging Potential effect on ability to dose or absorption profile by Arrhythmia theoretical route of administration for epinephrine Nasal symptoms /
rhinitis 4.22% Loss of consciousness Anaphylaxis Symptom US % Intranasal Sublingual Oral* Inhalation* Confusion/somnolence Analysis of anaphylaxis Respiratory failure symptom frequency in the Stridor 1-13 Diarrhea Nasal symptoms / rhinitis 4% X X
USA (n = 4,805 patients) Abdominal pain or cramping Chest tightness / Chest pain Oropharyngeal edema 10% X X X Orophyarngeal Edema 9.66% Nausea Vomiting / Emesis 20% X X X Cough Hypotension Dysphagia 23% X X Presyncope / Dizziness /Light headedness
Hoarseness Laryngeal Edema 24% X X Diarrhea + Abdominal Pain Vomiting / Emesis 20.01% Throat pruritus Bronchospasm 24% X Dysphagia 23.32% Laryngeal Edema 23.58% Intraoral Edema or 24% X X X Bronchospasm 23.79% Tongue Swelling Intraoral Edema or
Tongue Swelling 24.38% Syncope/Presyncope Angioedema (e.g. face, Tachycardia 45% X X X Wheezing lips, tongue or larynx) Throat Tightness Angioedema (unspecified) 45.12% Difficulty Breathing / Pruritus 55% X Flushing Dyspnea Urticaria *insufficient
oral and inhalation systemic absorption due to rapid conjugation and Difficulty Breathing / Dyspnea 55.23% 14 oxidation in GI tract or difficulty taking in enough puffs Urticaria/Angioedema 0% 20% 40% 60% 80% 100% References: 1. Pistiner M, et al. J
Allergy Clin Immunol Pract. 2021. 2. Jalil M, et al. Abstract at AAAAI 2020 Virtual Meeting. 3. Gonzelez-Estrada A, et al. Ann Allergy Asthma Immunol. 2018. 4. Lee S, et al. J Allergy Clin Immunol. 2017. 45 5. Lee S, et al. J Allergy Clin Immunol
Pract. 2014. 6. Manivannan V, et al. Am J Emerg Med. 2014. 7. Wood RA, et al. J Allergy Clin Immunol 2014. 8. Walsh KE, et al. Pharmacoepidemiol Drug Saf 2013. 9. Decker WW, et al. J Allergy Clin Immunol. 2008. 10. Ross MP, et al. J Allergy Clin
Immunol. 2008. 11. Webb LM & Lieberman P. Ann Allergy Asthma Immunol. 2006. 12. Ditto AM, et al. Ann Allergy Asthma Immunol. 1996. 13. Rudders SA, et al. Pediatrics. 2010.14. Simons KJ, et al. J Allergy Clin Immunol. 2004. Note that some
publications do not specify angioedema symptom subtype. Angioedema subtype frequency aggregated when reported.

Excellent Tolerability and Palatability Adverse events generally mild
in nature with no meaningful nasal irritation or pain up to 4 mg dose No serious adverse events in any clinical study No risk of needle-related injuries or blood vessel injections with neffy Most common adverse events (>5%) were mild nasal
discomfort (9.7%) and mild headache (6%), with no correlation of nasal discomfort to pain or irritation Ø Mean VAS pain scores between 5 to 8 out of 100 (no stinging or burning) Ø No irritation based on formal assessment (no erythema or
ulcers) Excellent palatability – no taste or smell with neffy 1 Ø “Inherent bitterness of epinephrine may hinder acceptability for patients, especially children” 46 References: 1. Rachid O, et al. AAPS PharmaSciTech.
2010.

Adverse Event Profile Compares Favorably to Autoinjectors Incidence of
adverse events in neffy, EpiPen and Auvi-Q studies (greater than 5% frequency) 1 2 2 Adverse Event 2 mg neffy 0.3 mg EpiPen 0.3 mg Auvi-Q Injection-site erythema 0% 32.6% 31.3% Injection-site pain 0% 24.4% 13.4% Tremors 0% 14.1% 13.4% Mild nasal
discomfort 9.7% 0% 0% Mild headache 6.0% <5% <5% Anxiety <1% 7.4% 10.4% Injection-site bleeding 0% 9.6% 4.5% Injection-site induration 0% 6.7% 4.5% 47 References: 1. FDA Advisory Committee, 2. Edwards ES, et al. Ann Allergy Asthma Immunol.
2013.

Low Dose is an Important Benefit of neffy that Minimizes Risk of
Overdosing, and Difficulty Monitoring Clinical Response Epinephrine has a therapeutic window and potential for overdose 1, 2 if too much is systemically absorbed too fast (e.g. IV bolus) – multiple cardiac events and fatalities 3, 4 reported
in literature 2 mg neffy has essentially minimal risk of overexposure even with higher bioavailability in the event of increased permeability during an allergic reaction or population variability (nasal abnormalities, impact of using other drugs or
substances on nasal mucosa, etc.) High dose of epinephrine can also lead to swallowing of non-absorbed 5, 6 epinephrine and GI side effects (vomiting/abdominal pain) Vomiting/abdominal pain is a common symptom of food-induced anaphylaxis (especially
biphasic) that can 7, 8, 9 confound monitoring of clinical response leading to unnecessary treatment and re-dosing neffy has minimal to no GI side effects References: 1. Casale TB, et al. Ann Allergy Asthma Immunol. 2024. 2. Ebisawa M, et al. J
Allergy Clin Immunol Glob. 2023. 3. Pumphrey RS, et al. Clin Exp Allergy. 2020. 4. Ring J, et al. Dtsch Arztebl Int. 2018. 5. Schlegel C, et al. J 48 Dtsch Dermatol Ges. 2009. 6. Dworaczyk D & Hunt A. Presentation at AAAAI 2023 (San Antonio,
Texas), 7. Francuzik W et al. J Allergy Clin Immunol. 2021. 8. Pflipsen MC & Colon KMV. Am Fam Physician. 2020. 9. Gupta, RS, et al. J Allergy Clin Immunol Pract. 2021.
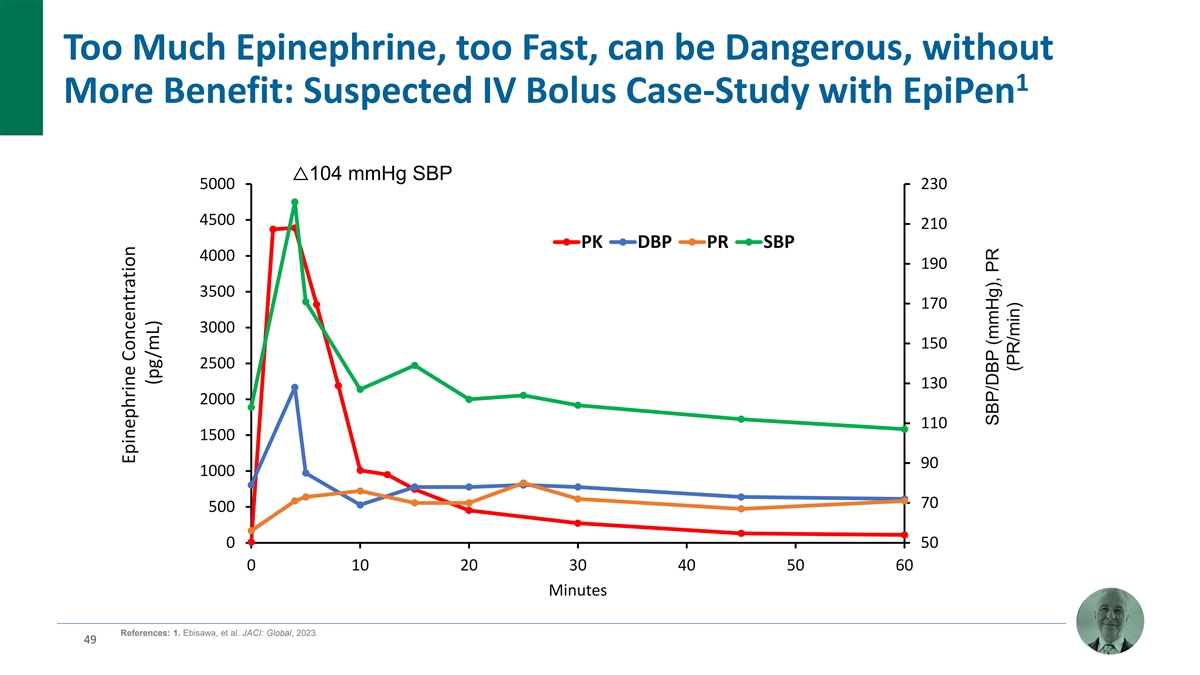
Too Much Epinephrine, too Fast, can be Dangerous, without 1 More
Benefit: Suspected IV Bolus Case-Study with EpiPen △104 mmHg SBP 5000 230 4500 210 PK DBP PR SBP 4000 190 3500 170 3000 150 2500 130 2000 110 1500 90 1000 70 500 0 50 0 10 20 30 40 50 60 Minutes References: 1. Ebisawa, et al. JACI: Global,
2023. 49 Epinephrine Concentration (pg/mL) SBP/DBP (mmHg), PR (PR/min)

Children more likely to experience vomiting and GI symptoms than adult
anaphylaxis patients with non-venom allergies ~40% rate of pediatric vomiting ~60% rate of pediatric GI symptoms Non-Venom in non-venom anaphylaxis in non-venom anaphylaxis Venom n = 7,217 n = 7,217 Age Age Important side effect to avoid for
monitoring of clinical outcomes (and also a co-morbidity that could alter absorption of dosing via mouth) References: 1. Francuzik W et al. J Allergy Clin Immunol. 2021. 50 Proportion Proportion
Human Factors Studies and Real-World Data Have Proven that neffy is
Easy for Patients to Carry and Simple to Administer Proven ease of use in human factors studies and real-world emergency use settings 100% of adults (including passersby without allergies) able to use neffy successfully without training 100% of
children (about half of the current autoinjector prescriptions) able to use neffy successfully without training Same device available over the counter in NARCAN OTC (no training required) 51

Patients Should be Carrying and Dosing Sooner with neffy’s
Potential Best-in-Class Epinephrine Product Profile Does it work? Will patients use it? Is it safe? Ø PK/PD response shows onset within 1 Ø Benign safety profile – mild Ø Benign safety profile – mild minute after dosing
nasal discomfort (9.7%) and nasal discomfort and headache mild headache (6%) Ø Rapid efficacy profile in OFC anaphylaxis Ø Palatable – no meaningful (100% response rate in first 15 min), as Ø No risk of injury (no needle)
pain/irritation, no taste/smell well as treatment-resistant urticaria and minimal risk of overdose even with Ø Small – fits in pocket Ø Predictable dose-proportional PK/PD population variability (high profile within range of approved
Ø Easy to use – 100% of adults bioavailability, low dose) injection products even under real- and children can use without world co-morbidities (e.g. rhinitis) Ø No side effects (GI, training (even passerby’s); vomiting,
erythema) that Ø Only anaphylaxis symptom that may ability to dose not obstructed could confound clinical alter PK/dosing is rhinitis, and for neffy, by anaphylaxis symptoms monitoring and treatment no negative impact on PK/PD 52
Commercial Opportunity Eric Karas Chief Commercial Officer
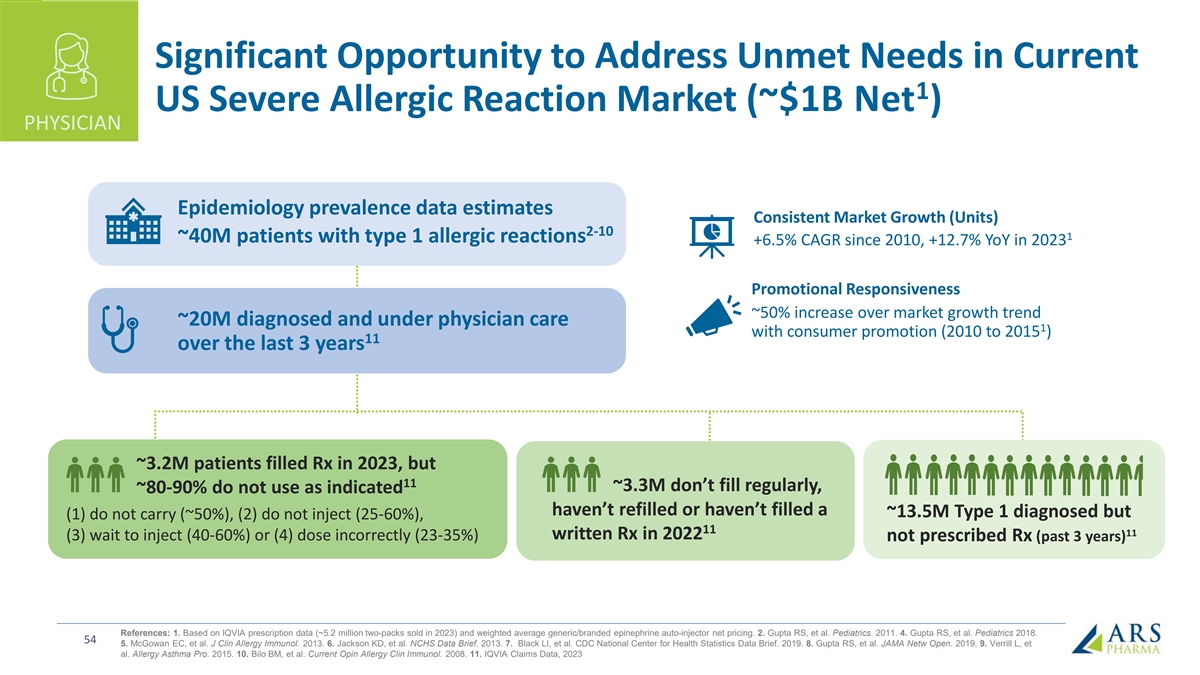
Significant Opportunity to Address Unmet Needs in Current 1 US Severe
Allergic Reaction Market (~$1B Net ) PHYSICIAN Epidemiology prevalence data estimates Consistent Market Growth (Units) 2-10 1 ~40M patients with type 1 allergic reactions +6.5% CAGR since 2010, +12.7% YoY in 2023 Promotional Responsiveness ~50%
increase over market growth trend ~20M diagnosed and under physician care 1 with consumer promotion (2010 to 2015 ) 11 over the last 3 years ~3.2M patients filled Rx in 2023, but 11 ~3.3M don’t fill regularly, ~80-90% do not use as indicated
haven’t refilled or haven’t filled a ~13.5M Type 1 diagnosed but (1) do not carry (~50%), (2) do not inject (25-60%), 11 11 written Rx in 2022 (3) wait to inject (40-60%) or (4) dose incorrectly (23-35%) not prescribed Rx (past 3 years)
References: 1. Based on IQVIA prescription data (~5.2 million two-packs sold in 2023) and weighted average generic/branded epinephrine auto-injector net pricing. 2. Gupta RS, et al. Pediatrics. 2011. 4. Gupta RS, et al. Pediatrics 2018. 54 5.
McGowan EC, et al. J Clin Allergy Immunol. 2013. 6. Jackson KD, et al. NCHS Data Brief. 2013. 7. Black LI, et al. CDC National Center for Health Statistics Data Brief. 2019. 8. Gupta RS, et al. JAMA Netw Open. 2019. 9. Verrill L, et al. Allergy
Asthma Pro. 2015. 10. Bilo BM, et al. Current Opin Allergy Clin Immunol. 2008. 11. IQVIA Claims Data, 2023
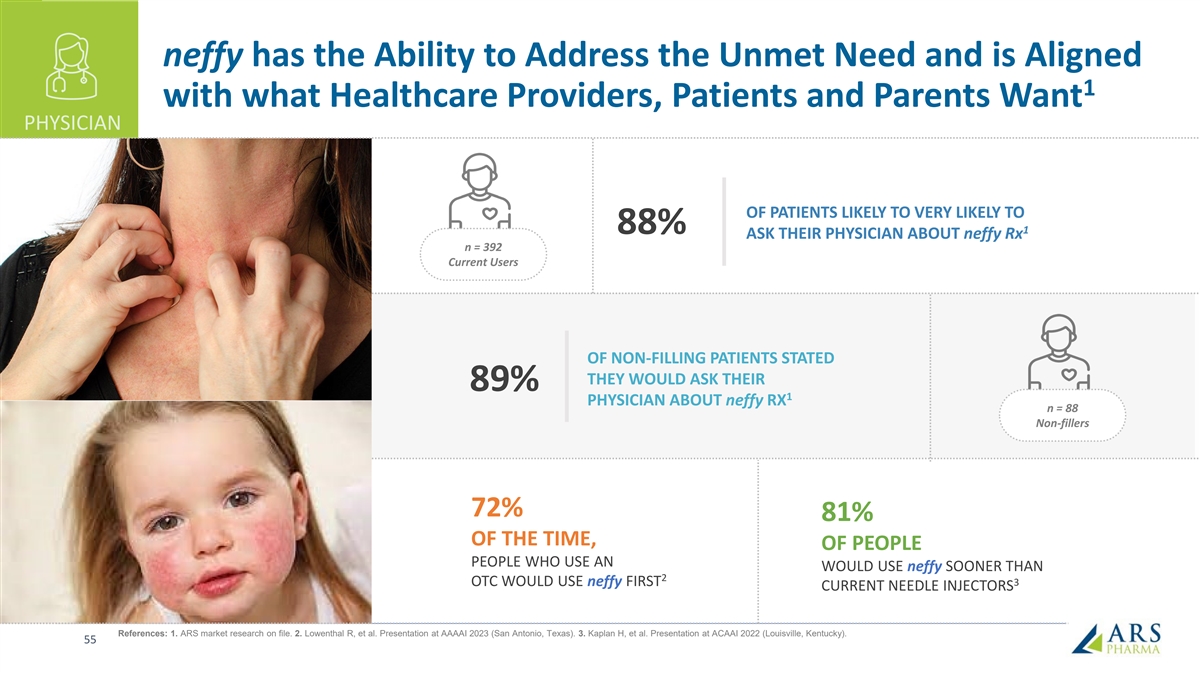
neffy has the Ability to Address the Unmet Need and is Aligned 1 with
what Healthcare Providers, Patients and Parents Want PHYSICIAN OF PATIENTS LIKELY TO VERY LIKELY TO 88% 1 ASK THEIR PHYSICIAN ABOUT neffy Rx n = 392 Current Users OF NON-FILLING PATIENTS STATED THEY WOULD ASK THEIR 89% 1 PHYSICIAN ABOUT neffy RX n =
88 Non-fillers 72% 81% OF THE TIME, OF PEOPLE PEOPLE WHO USE AN WOULD USE neffy SOONER THAN 2 OTC WOULD USE neffy FIRST 3 CURRENT NEEDLE INJECTORS References: 1. ARS market research on file. 2. Lowenthal R, et al. Presentation at AAAAI 2023 (San
Antonio, Texas). 3. Kaplan H, et al. Presentation at ACAAI 2022 (Louisville, Kentucky). 55
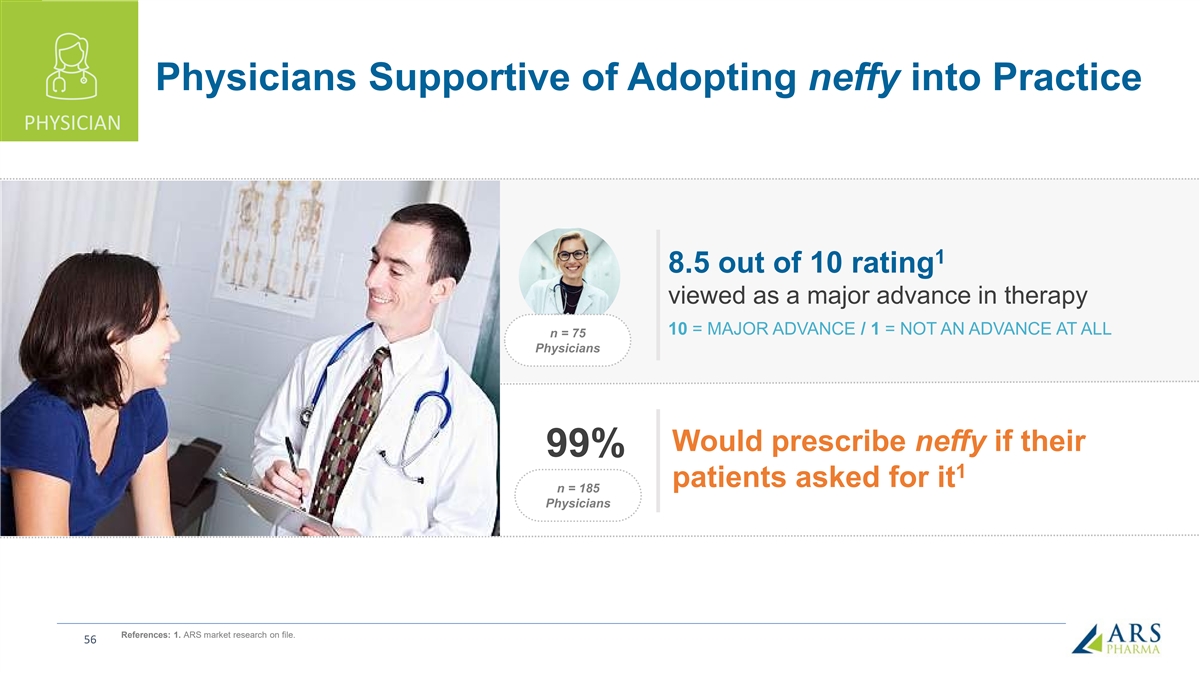
Physicians Supportive of Adopting neffy into Practice PHYSICIAN 1 8.5
out of 10 rating viewed as a major advance in therapy 10 = MAJOR ADVANCE / 1 = NOT AN ADVANCE AT ALL n = 75 Physicians Would prescribe neffy if their 99% 1 patients asked for it n = 185 Physicians References: 1. ARS market research on file.
56

Two-Thirds of Allergists and Half of GPs Ready to Prescribe neffy as
Soon as Possible; Majority of Pediatricians Expected PHYSICIAN to Prescribe within One Year Timeline for Prescribing neffy – % of physicians As soon as possible 68% Within one year of its approval 54% 52% 43% 1-3 years of it being on the
market 40% 30% After it is on the market for more than 3 years 5% General Allergists Pediatricians Practitioners (n=98) (n=56) (n=48) References: ARS market research on file. 57

neffy: Innovative Treatment to Overcome Known Challenges with
Needle-Injectors for SAR Patients PATIENT 45% REDUCTION IN TIME TO USE % of Time Carrying Average Time (minutes) at least One 1 from Symptom Start to Device Use 2,3 Epinephrine Device Benefits of needle-free 8.8 alternative to address major unmet
needs 9.3 % 55 Ø More allergy patients and Patient Carry 5.1 caregivers are likely to N = 100 2 N = 917 carry neffy compared to 4.9 current needle-bearing options 8.3 Ø Patients are likely to dose % neffy more rapidly with a Caregiver 4.7
85 N = 100 needle-free device Would Carry 3 N = 150 N = 200 Current Device neffy Market Research References: 1. Kaplan H, et al. Presentation at ACAAI 2022 (Louisville, Kentucky). 2. Warren CM, et al. Ann Allergy Asthma Immunol. 2018. 3. ARS market
research on file. 58

~ 72% of Respondents would Make a Special Appointment to Discuss neffy
with their HCP PATIENT Action Taken to Discuss 49% neffy with HCP 45% 40% Make a special in-person appointment to discuss neffy 27% 27% 27% 26% Make a special telehealth 22% appointment to discuss neffy 18% Wait until my next regular appointment to
discuss neffy 6% 6% 6% Wait to see if my doctor wanted to discuss neffy with me Total Patient (P) Caregiver (C) Respondents who may ask their HCP about neffy, Aug-23: Total (n=476), Patient (n=244), Caregiver (n=232) % of respondents References: ARS
market research on file. 59

60

neffy Strategic Objectives EDUCATE PRESCRIBERS Drive adoption within
specialty and high decile prescribers on the compelling value-proposition of neffy FACILITATE ACCESS neffy access, affordability and support services ACTIVATE PATIENTS Create awareness and motivate patients and caregivers to seek neffy 61

Drive Adoption within Specialty and High Decile Prescribers EDUCATE
Healthcare Provider Launch Objectives Ø Commercial force of 110 Sales and Virtual Representatives and Area Sales Managers Ø Education, awareness, and resources to drive adoption (neffy Experience) Ø Calling on 12,500 Allergy
Specialists and High Decile Prescribers • Reaching 40-45% of Prescriptions from all HCPs • Reaching >80% of Prescriptions from Allergists and Pediatricians 62

Committed to Ensuring neffy Access for all Patients FACILITATE Key
findings from discussions with the major payers and PBMs: • High degree of interest in neffy and positive receptivity in early conversations; proactively requesting clinical presentations prior to approval • Epinephrine is covered as a
pharmacy benefit, and we expect to achieve coverage without restriction for 80% of commercial lives within a year of launch • ARS is committed to access and affordability – we will offer a co-pay buydown to $25 for commercial patients, a
cash price of $199, and a Patient Assistance Program for uninsured or underinsured • neffyconnect will assist in managing coverage by providing patients, caregivers and healthcare providers with information regarding support programs and
financial aid “This is a game-changer; it really “There is no value in delaying access “If this is priced properly, addresses the unmet needs we currently to a product like this and nothing to this could be a
‘state-of-the-art have in this space, specifically the safety prior authorize (PA). We can’t PA if therapy’ for patients.” and tolerability issues.” the patient needs it.” – PBM – Payer – PBM
63
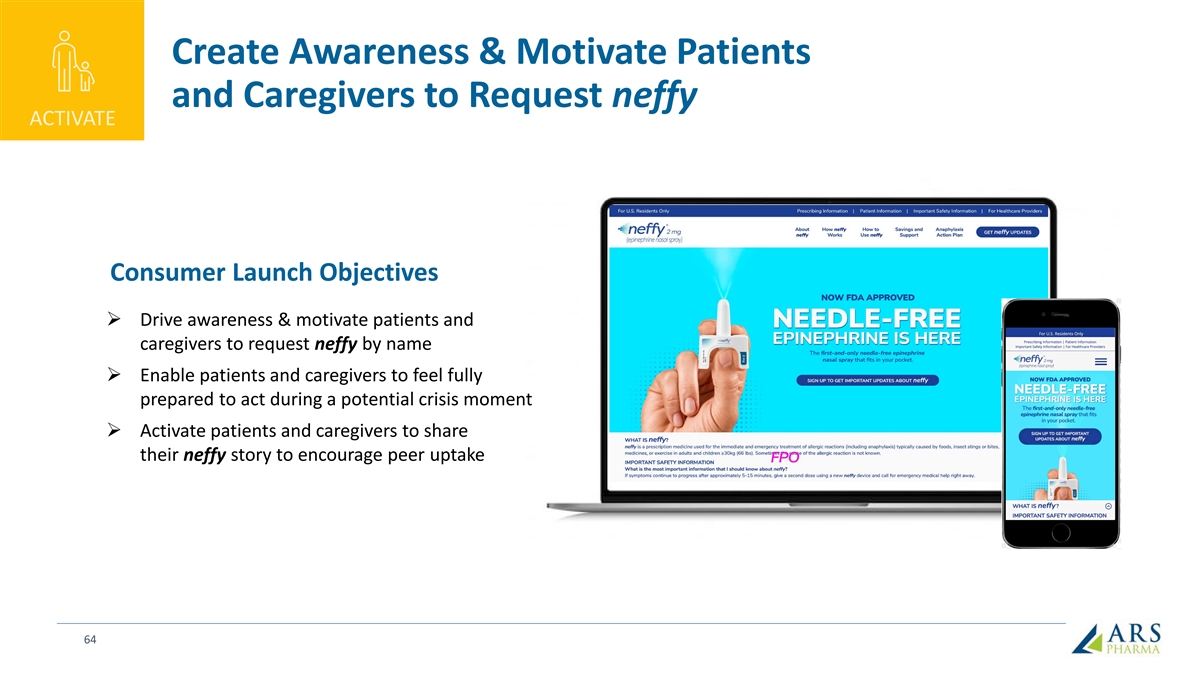
Create Awareness & Motivate Patients and Caregivers to Request
neffy ACTIVATE Consumer Launch Objectives Ø Drive awareness & motivate patients and caregivers to request neffy by name Ø Enable patients and caregivers to feel fully prepared to act during a potential crisis moment Ø Activate
patients and caregivers to share their neffy story to encourage peer uptake 64
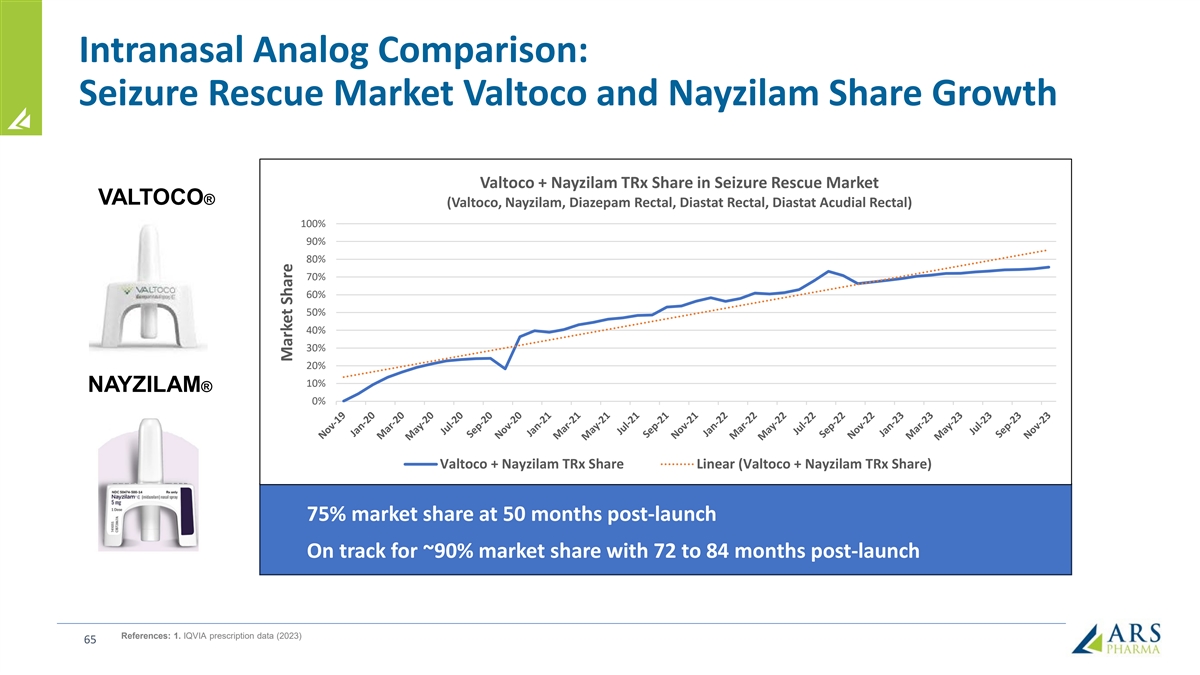
Intranasal Analog Comparison: Seizure Rescue Market Valtoco and
Nayzilam Share Growth Valtoco + Nayzilam TRx Share in Seizure Rescue Market VALTOCO® (Valtoco, Nayzilam, Diazepam Rectal, Diastat Rectal, Diastat Acudial Rectal) 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% NAYZILAM® 0% Valtoco + Nayzilam TRx
Share Linear (Valtoco + Nayzilam TRx Share) 75% market share at 50 months post-launch On track for ~90% market share with 72 to 84 months post-launch References: 1. IQVIA prescription data (2023) 65 Market Share
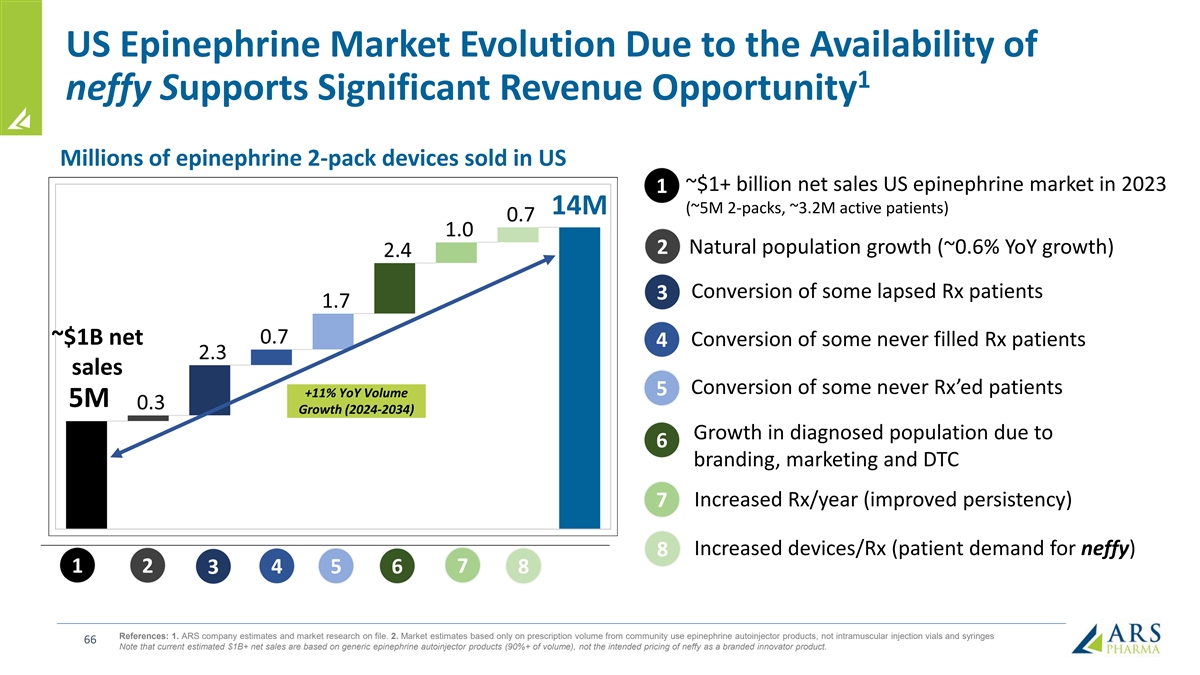
US Epinephrine Market Evolution Due to the Availability of 1 neffy
Supports Significant Revenue Opportunity Millions of epinephrine 2-pack devices sold in US ~$1+ billion net sales US epinephrine market in 2023 1 (~5M 2-packs, ~3.2M active patients) 14M 2 Natural population growth (~0.6% YoY growth) Conversion of
some lapsed Rx patients 3 ~$1B net Conversion of some never filled Rx patients 4 sales Conversion of some never Rx’ed patients 5 +11% YoY Volume 5M Growth (2024-2034) Growth in diagnosed population due to 6 branding, marketing and DTC
Increased Rx/year (improved persistency) 7 Increased devices/Rx (patient demand for neffy) 8 1 2 7 3 4 5 6 8 References: 1. ARS company estimates and market research on file. 2. Market estimates based only on prescription volume from community use
epinephrine autoinjector products, not intramuscular injection vials and syringes 66 Note that current estimated $1B+ net sales are based on generic epinephrine autoinjector products (90%+ of volume), not the intended pricing of neffy as a branded
innovator product.

neffy: the first needle-free way to administer epinephrine Rapid,
reliable delivery Small and easy to carry Place and Press administration Well-tolerated in extensive trials AVOIDS ALL NEEDLE-RELATED ADVERSE EVENTS

Financial Update *Post-Marketing Requirements/Post-Marketing
Commitments
Financial highlights Cash and short-term investments: $228M Debt: $0M
Common Shares: 96.4M As of 12/31/2023 Estimated at least three years of operating runway including the anticipated launch and commercialization of neffy 69

Significant Ex-US opportunity for neffy <10% TYPE I ALLERGY MARKET
PENETRATION (LESS THAN HALF OF US Europe EAI Market: ADOPTION RATES) ~$219M TODAY Japan EAI Market: ~$12M TODAY Canada EAI Market: ~$67M TODAY China EAI market: no approved products Significant Potential AUS/NZ EAI market: ~$18M TODAY 70 Source:
2023 IQVIA MIDAS (USD MNF)

Significant Catalysts for neffy in 2024 o US NDA response to CRL by
early Q2 2024 FDA o PDUFA action date anticipated in H2 2024 o EMA decision (CHMP Opinion) expected by mid-2024 EMA o China NDA filing expected by YE 2024 o Japan NDA filing expected by YE 2024 o Planning in progress for filing in other major ex-US
regions including Canada o Expansion opportunities • Positive data from Phase 2 chronic urticaria study reported in Feb 2024 • Initiation of Phase 2b outpatient urticaria study 71

Q&A
v3.24.0.1
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
ARS Pharmaceuticals (NASDAQ:SPRY)
Gráfico Histórico do Ativo
De Out 2024 até Nov 2024

ARS Pharmaceuticals (NASDAQ:SPRY)
Gráfico Histórico do Ativo
De Nov 2023 até Nov 2024

